1. DEFINITION & ANATOMY
Lower back pain is one of the most common conditions affecting people of all ages. Your lower back, or lumbar spine, is a strong, complex structure made up of five vertebrae (L1–L5), shock-absorbing intervertebral discs, small facet joints that guide movement, and a network of ligaments. Key muscles like the deep multifidus, larger erector spinae, and powerful glutes work together to support and move your spine.

Low back pain can be broadly categorised:
Mechanical or Non-Specific Low Back Pain: The most common type, involving pain from the joints, muscles, or ligaments without a specific structural cause.
Disc-Related Pain: Pain arising from an intervertebral disc, which can sometimes bulge or herniate.
Nerve Root Irritation (Sciatica): When a nerve root is compressed or irritated as it exits the spine, causing pain, pins and needles, or numbness down the leg.
Facet Joint Pain: Pain originating from the small stabilising joints on the back of the spine.
Sacroiliac (SI) Joint Pain: Pain from the large joint connecting your spine to your pelvis.
Piriformis Syndrome: A specific condition where the sciatic nerve is irritated or compressed as it passes by or through the piriformis muscle deep in the buttock, mimicking sciatica.
A physiotherapist can accurately diagnose the primary source of your pain and create a targeted treatment plan.
2. SYMPTOMS & SIGNS
Back-dominant vs. Leg-dominant Pain: Pain can be felt mainly in the lower back, or predominantly in the buttock and leg.
Sharp Pain: Often felt with specific movements like bending forward, lifting, or twisting.
Dull Ache: A common symptom after prolonged sitting, driving, or standing.
Morning Stiffness: Difficulty moving or significant soreness upon waking that eases with gentle movement.
Pain on Extension: Discomfort when arching backwards or standing for long periods.
Buttock & Leg Pain: A deep ache in the buttock that may radiate down the back of the thigh, typical of piriformis syndrome or sciatica.
Neural Symptoms: Pins and needles, numbness, or weakness in the leg or foot.
Sitting Aggravation: Pain that worsens with sitting, especially in soft chairs or during driving. Many find relief with standing or walking.
Antalgic Posture: You might find yourself leaning to one side to relieve pressure and pain.
Limited Movement: Difficulty bending forward to touch your toes or extending backwards.
Local Tenderness: The area over your buttock or piriformis muscle may be very tender to touch.
Positive Neural Tension Signs: Tests like the Straight Leg Raise (SLR) or Slump test may reproduce your leg symptoms.
3. CAUSES & RISK FACTORS
Prolonged Sitting & Desk Work: Sustained postures increase load on discs and surrounding muscles.
Deconditioning: A lack of general fitness and poor core or gluteal muscle strength.
Sudden or Awkward Lifting: A sudden, heavy load or using poor lifting mechanics can cause acute injury.
Repetitive Bending or Twisting: Common in manual jobs or certain sports.
Previous Episodes of Back Pain: A major predictor of future episodes.
Poor Sleep & High Stress: These factors can heighten pain sensitivity and impair muscle recovery.
Pregnancy & Postpartum Changes: Hormonal shifts and changes in body mechanics increase strain on the back and pelvis.
Generalised Joint Hypermobility: Can lead to reduced joint stability.
High-Load Sports: Activities involving repeated impact or rotation, like running or golf.
Changes in Footwear or prolonged walking on hard surfaces.
Wallet Neuropathy: Sitting on a bulky wallet in your back pocket can directly compress the piriformis muscle and sciatic nerve.
Anatomical Variations: In some people, the sciatic nerve passes directly through the piriformis muscle, making it more susceptible to irritation.
4. HOW PHYSIOTHERAPY HELPS
Assessment: We perform a thorough assessment to screen for any red flags and classify the main driver of your pain. This includes examining your movement patterns, muscle strength, hip mobility, and neural tension. We will liaise with your GP if further investigation is needed.
Manual Therapy: We use hands-on techniques such as joint mobilisations for the lumbar spine and SI joint, and soft-tissue release for tight paraspinal muscles, glutes, and the piriformis. Where appropriate, we may also use gentle nerve gliding techniques.
Exercise Therapy: You will receive a graded exercise programme tailored to your needs. This may include mobility drills, core control exercises targeting deep stabilisers (multifidus, transverse abdominis), and strengthening for the hips and glutes. As you improve, we introduce progressive loading with movements like hinges, squats, and carries. For certain conditions, we may use McKenzie-style exercises that focus on a preferred direction of movement.
Education & Habit Change: Understanding your pain is key. We provide education on pain science, strategies for pacing your activity, and advice on taking regular breaks from sitting. We also offer ergonomic guidance for your workstation, advice on sleep positions, and simple tips like removing your wallet from your back pocket.
Adjuncts: We may use taping for postural feedback or short-term pain relief, alongside guidance on using heat or ice. We can also collaborate with your GP regarding pain medication if required.
5. TIMELINE / EXPECTED RECOVERY
Non-Specific/Mechanical Pain: Most acute episodes show significant improvement within 2–6 weeks with consistent physiotherapy and adherence to your home exercise programme.
Disc or Radicular Pain: These conditions can take longer to resolve, often requiring 6–12 weeks or more for the nerve to settle and strength to be fully restored.
Piriformis Syndrome: Typically responds well to targeted treatment within 4–8 weeks, provided contributing factors like sitting habits are addressed.
Flare-ups are common with back pain, but the goal of physiotherapy is to equip you with the self-management skills to control them quickly and effectively. Progressive loading and building resilience is crucial for long-term success.
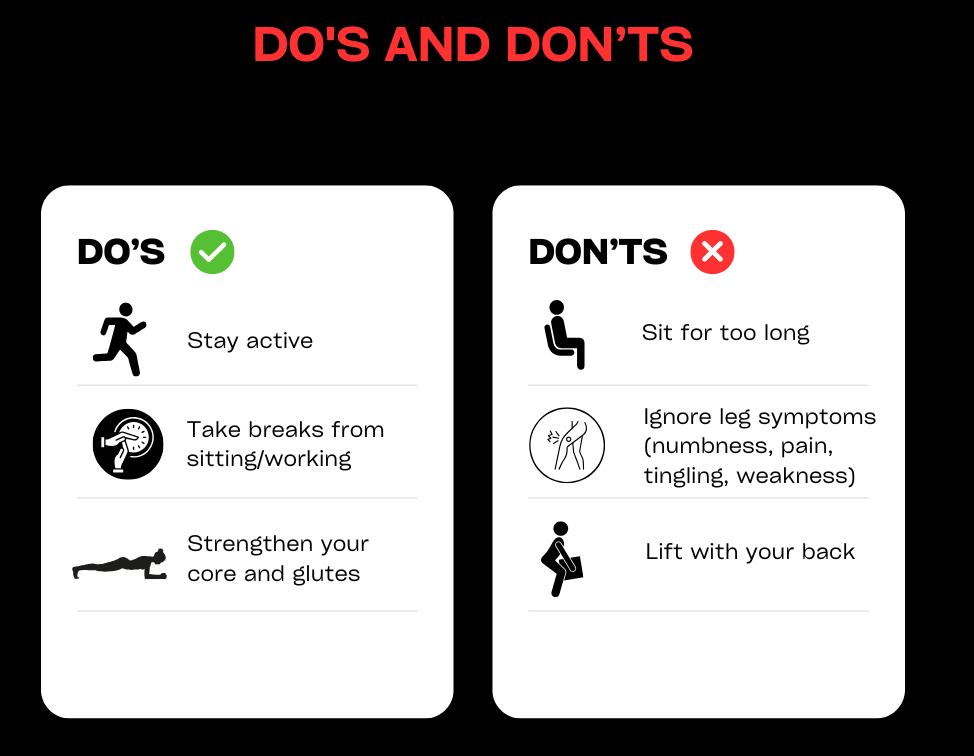
6. SELF-HELP & PREVENTION
During a Flare-up: Aim for relative rest. Avoid provocative movements like deep bending and prolonged sitting. Use a heat pack for muscle ache or an ice pack for sharp, acute pain.
Gentle Movement is Key: Perform gentle mobility exercises like pelvic tilts and single knee-to-chest hugs. Try short, frequent walks on flat ground as tolerated. A gentle piriformis stretch can also be helpful.
Take Posture Breaks: Use the 20-8-2 rule at your desk: for every 20 minutes of sitting, stand for 8 and move for 2.
Learn to Hinge: Practise bending from your hips while keeping a neutral spine for tasks like loading the dishwasher or picking things up.
Optimise Your Sleep: Try sleeping on your side with a pillow between your knees or on your back with a pillow under your knees to support your spine.
Build a Routine: Incorporate regular walking and a simple strengthening programme for your core, hips, and glutes 2–3 times per week to build resilience.
Manage Stress & Sleep: Prioritise good sleep hygiene and use stress management techniques, as these have a direct impact on pain.
7. WHEN TO SEE A PHYSIO OR SPECIALIST
If you feel in doubt about your diagnosis or your lower back problem is not resolving book a physiotherapy assessment with one of our physiotherapists.
In the UK, up to 80% of people will experience back pain during their lifetime (NICE.org.uk). This equates to almost £5bn per annum through missed days of work, reduced hours or decreased productivity (britishpainsociety.org). Back pain can be split into several sub-categories – from disc related pain, mechanical (or muscle and joint) pain, neurogenic (nerve) pain, and metastatic (cancer) pain. At W5Physio, we’ll quickly diagnose your back pain before tailoring treatment to your specific needs. You don’t need to live with lower back pain. Get in touch with us today.